Semen Analysis
Evaluation of male fertility is done due by checking the semen in the lab. In our andrology lab the embryologist does the semen analysis. It is done to check the no of sperms, the motility of sperms, presence of abnormal sperms and several other parameters.
| Semen Abnormalities | ||
|---|---|---|
| A | Normozoospermia | Normal ejaculate |
| B | Oligozoospermia | Sperm concentration Less than 20 million/mL |
| C | Asthenozoospermia | movement abnormalities |
| D | Teratozoospermia | Less than 30% sperm with normal morphology |
| E | Oligoasthenoteratozoospermia | Disturbance of all three variables |
| F | Azoospermia | No sperm ejaculate |
| G | Aspermia | No ejaculate |


Common cause of abnormalities:
- Artefact :(incorrect collection/examination methodology)
- Reddish color: Hemospermia- trauma, inflamation or tumor of the genital tract
- Highly viscous semen: Cause is not known (impaired motility)
- Liquefation Failure: (impaired motility)-impaired prostate function
- Increased Semen volume:Hyperspermia-more than10ml may cause dilutional oligozoospermia
Aspermia:
Absence sperms in the ejaculate- Retrogade ejaculation-in bladder
- An ejaculation- problem with ejaculation
- Bilateral ejaculatory duct obstruction
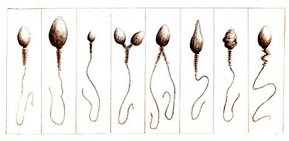
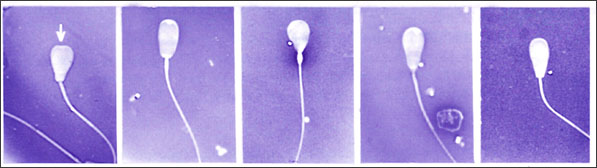
Structure of Abnormal Sperm
- Sperm concentration
-
Oligozoospermia (Reduced Count):
If less than 20 million / ml-oligozoospermia (repeat semen analysis after 3 months: 74 days for process of spermatogenesis and 12 / 20 days for travel) - Azoospermia( Absence of Sperm):
- No spermatozoa in the fresh or centrifuged resuspended semen sample
- Polyzoospermia (Increased sperm)
- If more than 350 million/ml
- Sperm motility (Reduced movement):
- If less than 50% progressively motile asthenozoospermia (EM-sperm tail defect).
- Necrozoospermia:
- Dead sperms
- Teratozoospermia (Abnormal Sperm):
- Presence of more than 70% abnormal sperm morphology in the sample.
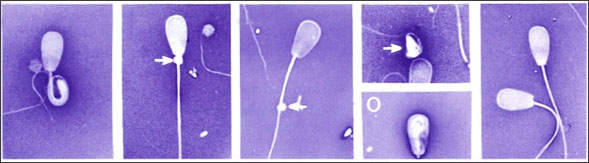
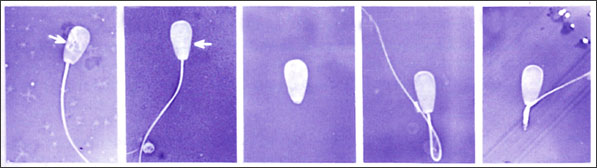
Abnormal sperms Microscopic view
Infertility Clinic
It has survived not only five centuries, but also the leap into electronic typesetting, remaining popularised only five Power of centuries.
- Learn moreHolistic Treatment
It has survived not only five centuries, but also the leap into electronic typesetting, remaining popularised only five Power of centuries.
- Learn moreSexual medicine
It has survived not only five centuries, but also the leap into electronic typesetting, remaining popularised only five Power of centuries.
- Learn moreSurrogacy Services
It has survived not only five centuries, but also the leap into electronic typesetting, remaining popularised only five Power of centuries.
- Learn moreSemen Analysis
Evaluation of male fertility is done due by checking the semen in the lab.
In our andrology lab the
embryologist does the semen analysis. It is done to check the no of sperms, the motility of sperms, presence
of abnormal sperms and several other parameters.
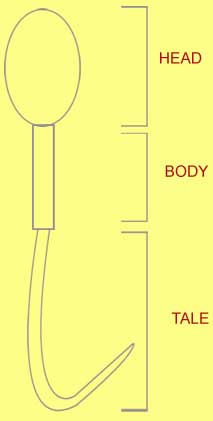
Structure of a Normal Sperm
| Semen Abnormalities | ||
|---|---|---|
| A | Normozoospermia | Normal ejaculate |
| B | Oligozoospermia | Sperm concentration Less than 20 million/mL |
| C | Asthenozoospermia | movement abnormalities |
| D | Teratozoospermia | Less than 30% sperm with normal morphology |
| E | Oligoasthenoteratozoospermia | Disturbance of all three variables |
| F | Azoospermia | No sperm ejaculate |
| G | Aspermia | No ejaculate |
Common cause of abnormalities:
- Artefact :(incorrect collection/examination methodology)
- Reddish color: Hemospermia- trauma, inflamation or tumor of the genital tract
- Highly viscous semen: Cause is not known (impaired motility)
- Liquefation Failure: (impaired motility)-impaired prostate function
- Increased Semen volume:Hyperspermia-more than10ml may cause dilutional oligozoospermia
Aspermia:
Absence sperms in the ejaculate
- Retrogade ejaculation-in bladder
- An ejaculation- problem with ejaculation
- Bilateral ejaculatory duct obstruction
Abnormal sperms Microscopic view
Structure of Abnormal Sperm
- Sperm concentration
-
Oligozoospermia (Reduced Count):
If less than 20 million / ml-oligozoospermia (repeat semen analysis after 3 months: 74 days for process of spermatogenesis and 12 / 20 days for travel) - Azoospermia( Absence of Sperm):
- No spermatozoa in the fresh or centrifuged resuspended semen sample
- Polyzoospermia (Increased sperm)
- If more than 350 million/ml
- Sperm motility (Reduced movement):
- If less than 50% progressively motile asthenozoospermia (EM-sperm tail defect).
- Necrozoospermia:
- Dead sperms
- Teratozoospermia (Abnormal Sperm):
- Presence of more than 70% abnormal sperm morphology in the sample.
